Lead a normal life with modern treatment for Crohn's disease (CED)
Living with a chronic inflammatory bowel disease
With Crohn's disease and other chronic inflammatory bowel diseases (IBD) such as ulcerative colitis, many sufferers are faced with one central question: Can I lead as normal a life as possible? Our answer at Vivomed - Gastroenterology Bern:
With early diagnosis, modern, guideline-based therapies and close-knit care, this is possible in most cases.
What is Crohn's disease?
Crohn's disease is a chronic, usually intermittent, transmural inflammation of the digestive tract. Typically affected are
- the terminal ileum (last section of the small intestine)
- the large intestine (colon)
In principle, however, any section from the mouth to the anus can be affected. The inflammation is transmural, i.e. it affects all layers of the intestinal wall and can lead to stenosis, fistulas and abscesses.
Crohn's disease is a type of IBD and is also known as regional enteritis, granulomatous ileitis or ileocolitis.
Typical symptoms of Crohn's disease
Not all patients have the same symptoms. Common signs of an attack are
- Chronic diarrhea (often without much blood)
- Abdominal pain and cramp-like symptoms
- Weight loss
- Loss of appetite
- Tiredness
- Fever and general feeling of illness
- Perianal complaints such as fissures, fistulas or abscesses in the anal area
- Extraintestinal manifestations may also occur, i.e. symptoms outside the bowel, e.g
- Joint inflammation and pain (arthritis, arthralgia)
- Skin changes (e.g. erythema nodosum, pyoderma gangraenosum)
- Eye inflammation (uveitis, iritis, episcleritis)
- Liver and biliary tract diseases (e.g. primary sclerosing cholangitis)
- Growth disorders and anemia in children and adolescents
In children in particular, general symptoms such as fever, anaemia or growth retardation may be prominent - even if abdominal pain and diarrhoea are not severe.
How is Crohn's disease diagnosed?
Crohn's disease is diagnosed clinically - there is no single "Crohn's lab" or "Crohn's exam". Typically we combine:
- Interview & physical examination
Detailed medical history (symptoms, duration, family history, smoking, medication)
Physical examination, assessment of abdomen, anus, joints, skin, etc. - Laboratory and stool tests
Inflammation values (e.g. CRP, BSG), blood count, iron status, vitamin B12, vitamin D, albumin - Stool tests for intestinal germs such as Clostridioides difficile
- Fecal calprotectin (FC) to differentiate between inflammatory vs. non-inflammatory causes of diarrhea
- Endoscopy (endoscopy)
- Ileocolonoscopy (colonoscopy with visualization of the terminal ileum): Removal of biopsies from affected and inconspicuous tissue, documentation of extent and severity
- oesophago-gastro-duodenoscopy (OGD) for complaints in the upper digestive tract
- Imaging
- MR or CT enterography to visualize the small intestine, stenoses, fistulas and abscesses
- Intestinal ultrasound (IUS) as a radiation-free, repeatable method for monitoring inflammation
- MRI of the pelvis or endosonography for perianal fistulas
- If an abscess or complicated course is suspected: CT/MR abdomen & pelvis
How can Crohn's disease progress if left untreated?
Crohn's disease begins with an inflammatory reaction of the crypts and with crypt abscesses that progress to small focal aphthoid ulcers. This mucosal damage can develop into deep longitudinal and transverse ulcers with intervening mucosal edema, creating the characteristic appearance of a cobblestone relief.
The transmural spread of the inflammation leads to lymphoedema and thickening of the intestinal wall and mesentery. The mesenteric fat typically spreads to the serosal surface of the intestine. The mesenteric lymph nodes are often enlarged. The pronounced inflammatory reaction can lead to hypertrophy of the musculares mucosae, fibrosis and stricture formation and thus to intestinal obstruction.
Abscesses occur frequently, fistulas often penetrate the adjacent structures, including other intestinal loops, the bladder or the psoas muscle. Fistulas can also extend into the skin of the anterior abdomen or into the flanks. Regardless of intra-abdominal disease activity, perianal fistulas and abscesses occur in 25-33% of cases and are often the most troublesome complications of Crohn's disease.
Noncaseating granulomas can occur in the lymph nodes, peritoneum, liver and all layers of the intestinal wall. Although their presence is pathognomonic, they are not found in about half of patients with Crohn's disease. The presence of granulomas does not appear to be associated with the clinical course of the disease.
The segments of the diseased bowel are sharply demarcated from the neighboring normal bowel (so-called skip areas), hence the name regional enteritis.
- About 35% of Crohn's disease cases affect the ileum alone (ileitis).
- About 45% involve the ileum and colon (ileocolitis), with a predilection for the right side of the colon.
- About 20% involve the colon alone (granulomatous colitis), most of which, unlike ulcerative colitis, exclude the rectum.
Occasionally, the entire small intestine is affected (jejunoileitis). The stomach, duodenum or oesophagus are rarely affected clinically, although microscopic evidence of the disease is often found in the gastric antrum, especially in younger patients. If no surgical intervention is performed, the disease almost never spreads to regions of the small intestine that were not affected at initial diagnosis.
Crohn's disease & other IBD: Who is affected?
Crohn's disease can occur at any age, but is more common between the ages of 17 and 40. Many patients are in young adulthood when the disease is diagnosed - a phase of life in which education, career and family planning play an important role. This makes good, forward-looking treatment planning all the more important.
How is Crohn's disease classified?
1. Crohn's disease is divided into three basic patterns:
- primarily inflammatory form, which after a course of several years usually develops into
- the mainly stenotic or obstructive form or
- the mainly penetrating or fistula-forming form.
These different clinical patterns require different therapeutic approaches. There is genetic data indicating a molecular basis for this classification.
2.The Montreal Classification classifies Crohn's disease as follows:
Age of manifestation
- A1: < 16 years
- A2: 17-40 years
- A3: > 40 years
Localization
- L1: Ileum (small intestine; part of the small intestine)
- L2: Colon (large intestine)
- L3: Ileocolic
- L4: Upper gastrointestinal tract (gastrointestinal tract)
Biological behavior
- B1: non-stretching, non-penetrating
- B2: structuring
- B3: internally penetrating
- B4: perianal-penetrating
This classification helps us to assess the risk of complications (e.g. stenoses, fistulas, operations) and to adapt treatment accordingly at an early stage.
Risk factors for an aggressive course are, for example
- young age at diagnosis
- extensive infestation, especially ileum/ileocolon
- perianal/severe rectal disease
- pronounced extraintestinal manifestations
- already penetrating or stricturing behavior at the time of diagnosis
3. Classification of severity
The Crohńs Disease Activity Index (CDAI) helps to determine the severity of the disease as it progresses. The following factors are recorded:
- Number of soft stools
- Intensity of abdominal pain
- Extraintestinal ("outside the bowel") manifestations
- Iritis (inflammation of the iris)/uveitis (inflammation of the middle skin of the eye, which consists of the choroid (choroida), the corpus ciliare and the iris)
- Stomatitis aphthosa ("mouth rot")
- Pyoderma gangraenosum (PG; synonym: ulcerative dermatitis) - sterile, destructive, neutrophil-rich and painful inflammation of the skin, in which ulceration (ulcer formation) and gangrene (tissue destruction due to ischemia or other damage) occur over a large area, usually in one place.Note: In up to 50 percent of cases, pyoderma gangraenosum is associated with a systemic disease (chronic inflammatory bowel disease (IBD), paraproteinemia, myeloproliferative and rheumatologic diseases).
- Erythema nodosum (synonyms: nodular erythema, dermatitis contusiformis, erythema contusiforme; plural: erythema nodosa) - granulomatous inflammation of the subcutis (subcutaneous fatty tissue), also known as panniculitis, and a painful nodule formation (red to blue-red color; later brownish). The overlying skin is reddened Localization: both sides of the lower leg, on the knee and ankle joints; less frequently on the arms or buttocks
- Arthralgia/arthritis (joint pain/joint inflammation)
- Anal fissure/anal fistula
- Other fistulas
- Temperature > 37 °C
- Symptomatic diarrhea treatment
- Resistance in the abdomen
- Hematocrit (proportion of erythrocytes (red blood cells) in the volume of blood)
- Body weight
- General condition
The Harvey-Bradshaw Index assesses the severity of symptoms in Crohn's disease, including abdominal pain, diarrhea, abdominal masses and general well-being.
M. Henriksen et al, Scand J Gastroenterol. 2007; 42: 602-610
Complications associated with Crohn's disease?
There is an increased risk of developing carcinomas in the affected segments of the small intestine. Patients with colonic involvement have an increased long-term risk of colorectal cancer, similar to ulcerative colitis, if the disease persists to the same extent and for the same duration.
Chronic malabsorption can lead to nutrient deficiencies, especially of vitamin D and B12.
Toxic megacolon is a rare but serious complication of ulcerative colitis. It is a clinical syndrome characterized by ileus and colonic dilatation, which can be detected by X-ray. Many cases require aggressive surgical treatment.
Symptoms and signs of Crohn's disease: an overview
The most common symptoms of Crohn's disease include:
- Chronic diarrhea accompanied by abdominal pain, fever, decreased appetite and weight loss.Abdominal tenderness and possibly a palpable mass.In general, more severe rectal bleeding rarely occurs unless there is isolated involvement of the colon, which can cause symptoms similar to ulcerative colitis. One third of patients suffer from perianal complications such as fissures and fistulas, which can sometimes be the dominant or even initial complaints, and children often present with extraintestinal manifestations, including arthritis, fever of unknown origin, anemia or growth retardation, although abdominal pain and diarrhea may not be present.
Symptoms may vary with relapses of the disease. Pain is common and can occur with both simple relapses and complicating abscesses. In severe relapses of inflammation or abscesses, patients often show marked tenderness, pain, guarding and a strong feeling of illness. Stenotic segments can lead to intestinal obstructions, which are manifested by abdominal cramps, flatulence, constipation and vomiting. Adhesions following previous surgery can also lead to intestinal obstruction, which often occurs suddenly, without the usual signs such as fever, pain and general malaise that typically accompany obstruction due to an inflammatory episode of Crohn's disease. Enterovesical fistulas can lead to blistering of the urine (pneumaturia), while draining cutaneous fistulas can occur. Free perforation into the abdominal cavity is rare.
This chronic disease can also cause a number of systemic symptoms, including fever, weight loss, malnutrition and various extraintestinal manifestations.
How is Crohn's disease diagnosed?
Crohn's disease is suspected in patients with inflammatory or obstructive symptoms or in patients without prominent gastrointestinal symptoms but with perianal fistulas or abscesses or with otherwise unexplained arthritis, erythema nodosum, fever, anemia or (in children) growth retardation. A positive family history of Crohn's disease increases suspicion.
Other gastrointestinal diseases, especially ulcerative colitis, may have similar findings and symptoms (e.g. abdominal pain, diarrhea). The differential diagnosis of ulcerative colitis can be problematic in the 20% of cases where Crohn's disease is confined to the colon. However, as the therapeutic approach is similar in both, the distinction only becomes important when surgery or experimental therapy is considered.
In patients with an acute abdomen (either initially or in the event of a relapse), abdominal overview radiographs in the supine and standing position and a CT abdomen are performed. These examinations reveal obstruction, abscesses or fistulas and other possible causes of an acute abdomen (e.g. appendicitis). With the help of ultrasound, a gynecological disease can be better differentiated in women with complaints in the lower abdomen and pelvis.
If the disease appears less acute, small bowel imaging with target images of the terminal ileum may be better than conventional CT. However, newer techniques of CT or MR enterography/enteroclysis, which combine high-resolution CT or MR imaging with contrast, are used. These imaging techniques are almost diagnostic when they show characteristic stenoses or fistulas with accompanying separation of bowel loops.
If the findings are equivocal, a CT double contrast enema or video capsule enteroscopy may show superficial aphthae and linear ulcers. A barium contrast enema may be used if the symptoms are predominantly attributed to the colon (e.g. diarrhea), it may show reflux of barium into the terminal ileum with irregularity, nodularity, stiffness, wall thickening and narrowed lumen. Differential diagnoses in patients with similar radiographic findings include carcinoma of the caecum, ileal carcinoid, lymphoma, systemic vasculitis, radiation enteritis, ileocecal tuberculosis and amoeboma.
In atypical or unclear cases (e.g. with diarrhea in the foreground and only minimal pain), a colonoscopy is performed in a similar way to suspected ulcerative colitis (including taking a biopsy, taking samples for intestinal pathogens and, if possible, viewing the terminal ileum). An endoscopic examination of the upper gastrointestinal tract(esophagogastroduodenoscopy (OGD)) can reveal subtle involvement of the stomach and duodenum even in cases where there are no symptoms of upper gastrointestinal tract involvement.
Technical investigations for Crohn's disease.
Laboratory tests should evaluate for anemia, hypoalbuminemia, and electrolyte disturbances. In patients with colonic involvement, elevated levels of alkaline phosphatase and gamma-glutamyltranspeptidase may indicate primary sclerosing cholangitis. Leukocytosis and elevated levels of acute phase proteins such as erythrocyte sedimentation rate and CRP may be non-specific signs, but may also serve as indicators of disease activity.
Vitamin D and B12 levels should be checked every 1-2 years to detect possible deficiencies. If deficiencies are suspected, additional laboratory tests for water-soluble vitamins (folic acid, niacin), fat-soluble vitamins (A, D, E, K) and minerals (zinc, selenium, copper) can be carried out.
All patients with inflammatory bowel disease should have their bone density monitored, usually by X-ray densitometry (DXA).
Perinuclear antineutrophil cytoplasmic antibodies are present in 60-70% of patients with ulcerative colitis, but only in 5-20% of patients with Crohn's disease. Anti-Saccharomyces cerevisiae antibodies are relatively specific for Crohn's disease, although they are not routinely used for diagnosis. Other antibodies such as anti-OmpC and anti-CBir1 are available, but their clinical utility is unclear; some studies suggest that high titers of these antibodies may have an unfavorable prognosis.
Prognosis in Crohn's disease: an overview
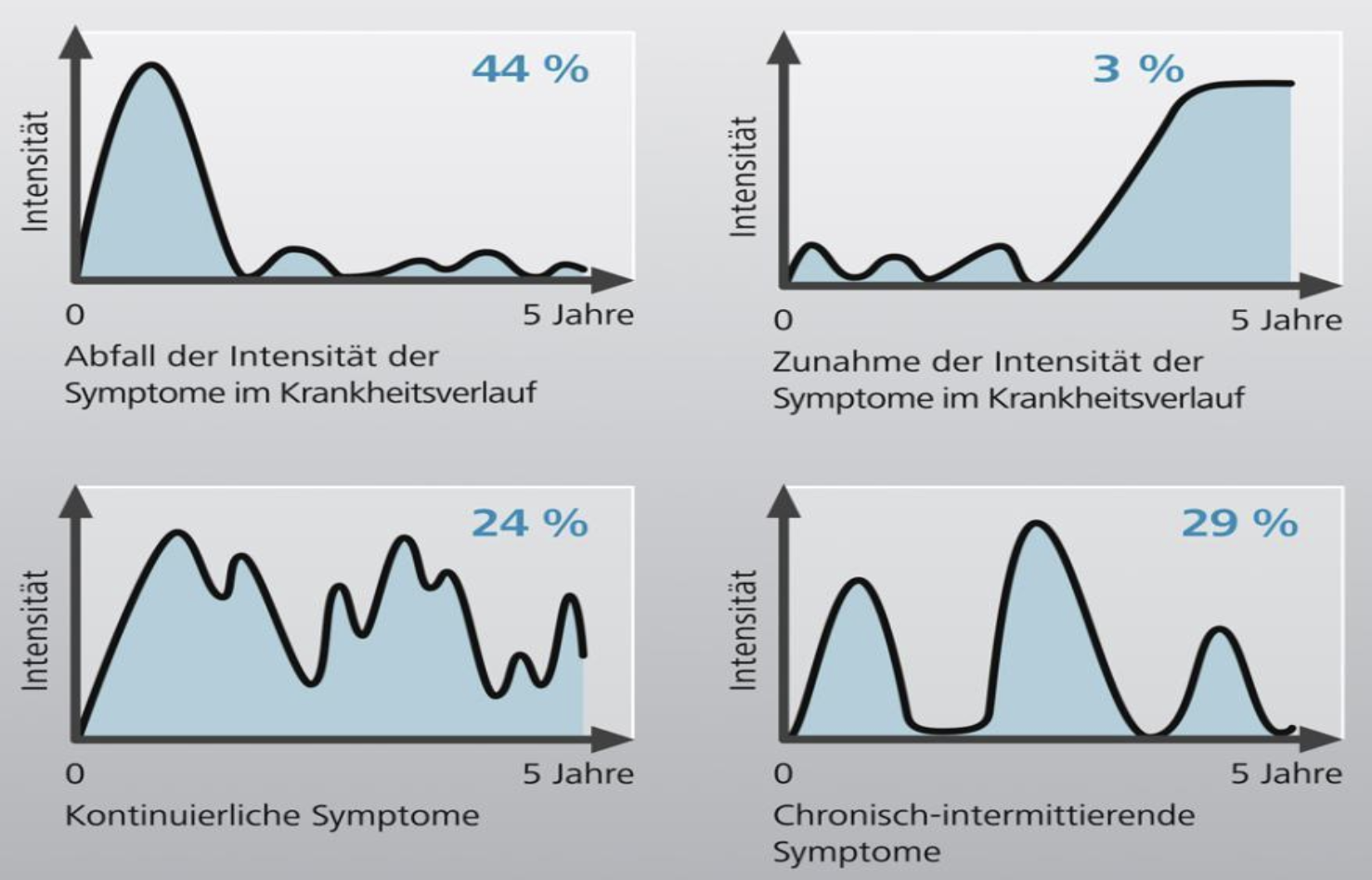
Crohn's disease is usually not curable, but is characterized by periodic relapses and remissions. Some patients experience severe disease progression with frequent episodes of pain, which can be very distressing.
Most patients can be successfully treated with appropriate medical therapy and, if necessary, surgical interventions. The disease-related mortality rate is very low. The most common cause of disease-related death is gastrointestinal cancer, especially colon and small bowel cancer. Thromboembolic complications, especially during active disease flares, can also be fatal. About 10% of people with Crohn's disease and its associated complications become permanently disabled.
Therapy for Crohn's disease - an overview
Treatment is individually adapted to your situation, the extent of the disease, its severity, previous treatments and life planning. We basically differentiate between
- Acute therapy ("induction") - Relapse treatment
- Maintenance therapy - Relapse prevention
1. General measures
- Stop smoking: Smoking worsens Crohn's disease and increases the risk of relapse and surgery.
- Optimize diet: Individual dietary recommendations depending on the findings; in the case of stenosis, adjust the diet if necessary.
- Correct deficiencies: e.g. iron, vitamin B12, vitamin D, folic acid, trace elements.
- Bone density monitoring (DXA): especially in the case of steroid therapy and long-term illness.
- Consider mental health: stress, depression and anxiety can influence relapses and should be actively treated.
2. Treatment of mild courses
For mild Crohn's disease and low risk of progression, the following strategies may be useful:
- Budesonide (controlled release, 9 mg/day) for mild to moderately active ileocecal infestation to induce remission.
- No routine long-term therapy with budesonide to maintain remission.
- Accompanying: nutritional therapy, monitoring (symptoms, calprotectin, imaging).
3. Treatment of moderate to severe courses
In moderately to severely active disease, biologics and small molecules are now often used at an early stage - not only after all conventional therapies have been exhausted.
Acute therapy (induction):
- Systemic corticosteroids (e.g. prednisone, Budenofalk) for short-term relapse therapy
In case of insufficient response or unfavorable risk profiles: - Anti-TNF antibodies
- Infliximab (Remicade)
- Adalimumab (Humira)
- Certolizumab pegol (Cimzia)
- Anti-integrin therapy
- Vedolizumab (Entyvio)
- Anti-interleukin-12/23 or anti-IL-23 antibodies
- Ustekinumab (Stelara)
- Risankizumab (SKYRIZI)
- Guselkumab (Tremfya)
- JAK inhibitors (small molecules)
- Upadacitinib (RINVOQ)
Maintenance therapy:
- Continuation of biologics or small molecules in an adjusted dosage
- if necessary, combination with immunomodulators (e.g. azathioprine, 6-mercaptopurine, methotrexate), in particular to reduce antibody formation against certain biologics
- Azathioprine/6-MP or methotrexate not as sole induction therapy in severe disease, but as an option for maintaining remission after steroid induction
Important:
Systemic corticosteroids are not suitable as long-term maintenance therapy - they increase the risk of osteoporosis, infections and other side effects.
4. Fistulating and stricturing Crohn's disease
For perianal fistulas and complicated courses:
- First: abscess drainage and, if necessary, seton placement (surgical relief)
- Supplementary
- Antibiotics (e.g. metronidazole, ciprofloxacin)
- Anti-TNF therapy (infliximab, adalimumab) - with proven efficacy in perianal fistulas
- vedolizumab, ustekinumab or upadacitinib for selected courses if necessary
- For stenoses
- Clarification of whether inflammatory or fibrotic predominance
- Inflammatory stenoses may respond to biologics/small molecules
- Pronounced fibrostenotic stenoses often require endoscopic dilatation or surgery
5. Surgical therapy
Around 30-50% of patients require at least one surgical procedure during the course of the disease. Typical reasons:
- repeated or severe intestinal obstruction (ileus)
- complex, unmanageable fistulas or abscesses
- Suspicion or detection of a carcinoma
Surgery can significantly improve quality of life, but does not cure Crohn's disease. A recurrence of inflammation in the area of the anastomosis (suture site) is possible.
Therefore, after surgery
- an early endoscopic check-up (6-12 months) and
- prophylactic drug therapy (e.g. anti-TNF, vedolizumab, metronidazole, thiopurine) in the case of risk factors
useful in order to recognize and prevent relapses in good time
Long-term risks & prevention
Patients with long-term Crohn's disease with colon involvement have an increased risk of colorectal cancer. We therefore recommend
- regular colonoscopic screening examinations with targeted biopsies
- individual intervals depending on duration, extent and inflammatory activity
The risk of small bowel cancer is increased in cases of small bowel involvement - careful clinical and imaging checks are important here.
Your advantage at Vivomed - Gastroenterology Bern
At Vivomed we combine:
- Current international guidelines with
- gentle, individually tailored treatment strategies
Our services for patients with Crohn's disease and other IBD:
- Detailed clarification of symptoms and risk profile
- Modern endoscopy (incl. ileocolonoscopy) and imaging
- Intestinal ultrasound for follow-up checks without radiation exposure
- Therapy planning with biologics and small molecules according to the latest evidence
- Close collaboration with surgery, radiology,
- Nutritional counseling and rheumatology
- Long-term support including preventive care,
- Vaccination advice and psychosocial support
Our aim is to work with you to find a way to control your disease as well as possible and enable you to lead an active, self-determined life.
When should you seek medical help?
Please contact us quickly if you:
- have persistent or increasing diarrhea
- Notice blood in your stool
- suffer from severe abdominal pain, fever or weight loss
- notice new perianal symptoms (swelling, pain, secretions)
- experience a significant relapse of your symptoms as a known IBD patient
Early action can prevent complications and improve treatment outcomes.
Conclusion
Crohn's disease can be challenging, but with a holistic approach and professional care, quality of life can be improved. Learn more about proven strategies for managing Crohn's disease and take an active role in your health.
Current treatment recommendations for biologics and small molecules (moderate to severe Crohn's disease).
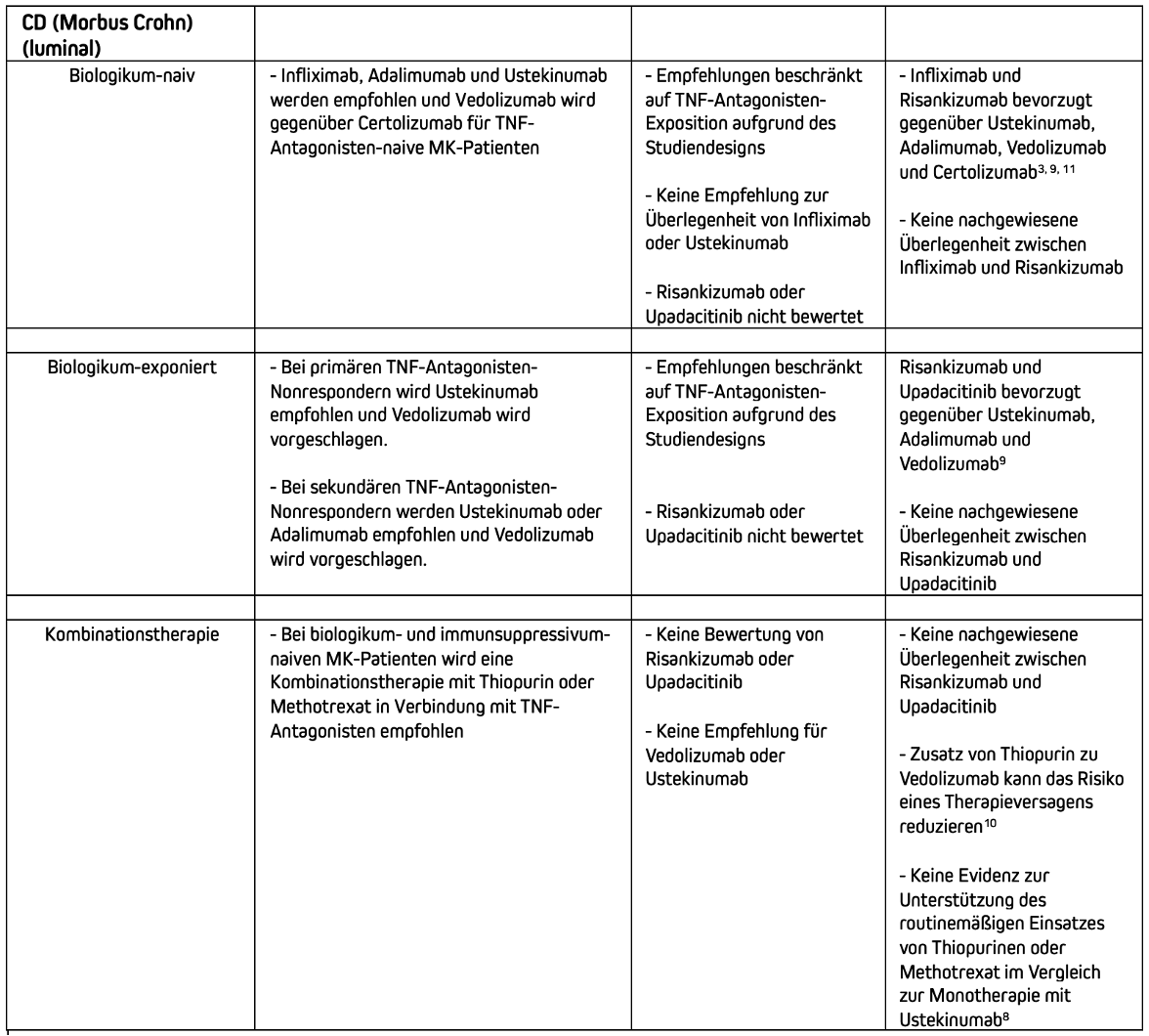
Treatment recommendations for biologics and small molecules (moderate to severe Crohn's disease).
1. Sands BE, Peyrin-Biroulet L, Loftus EV Jr, et al. Vedoli-zumab versus adalimumab for moderate-to-severe ulcerative colitis. N Engl J Med 2019;381:1215-1226.
2. Narula N, Wong ECL, Marshall JK, et al. Comparative efficacy for infliximab vs vedolizumab in biologic naive ulcerative colitis. Clin Gastroenterol Hepatol 2022;20:1588-1597 e3.
3. Narula N, Wong ECL, Dulai PS, et al. Comparative effectiveness of biologics for endoscopic healing of the ileum and colon in Crohn's disease. Am J Gastroenterol 2022;117:1106-1117.
4. Lasa JS, Olivera PA, Danese S, et al. Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol 2022;7:161-170.
5. Burr NE, Gracie DJ, Black CJ, et al. Efficacy of biological therapies and small molecules in moderate to severe ulcerative colitis: systematic review and network meta-analysis. Gut 2022;71:1976-1987.
6. Kochhar GS, Desai A, Farraye FA, et al. Efficacy of bio-logic and small molecule agents as second-line therapy after exposure to TN inhibitors in patients with ulcerative colitis: a propensity-matched cohort study. Aliment Pharmacol Ther 2023;58:297-308.
7. Yzet C, Diouf M, Singh S, et al. No benefit of concomitant immunomodulator therapy on efficacy of biologics that are not tumor necrosis factor antagonists in patients with inflammatory bowel diseases: a meta-analysis. Clin Gastroenterol Hepatol 2021;19:668-679.
8.Hu A, Kotze PG, Burgevin A, et al. Combination therapy does not improve rate of clinical or endoscopic remission in patients with inflammatory bowel diseases treated with vedolizumab or ustekinumab. Clin Gastroenterol Hepatol 2021;19:1366-1376.
9. Barberio B, Gracie DJ, Black CJ, et al. Efficacy of biological therapies and small molecules in induction and maintenance of remission in luminal Crohn's disease: systematic review and network meta-analysis. Gut 2023; 72:264-274.
10. Kirchgesner J, Desai RJ, Schneeweiss MC, et al. Decreased risk of treatment failure with vedolizumab and thiopurines combined compared with vedolizumab mon-otherapy in Crohn's disease. Gut 2022;71:1781-1789.
11. Wong ECL, Dulai PS, Marshall JK, et al. Comparative efficacy of infliximao vs ustekinumab for maintenance of clinical response in biologic naïve Crohn's disease. Inflamm Bowel Dis 2023;29:1015-1023.