Pfeiffer's glandular fever (infectious mononucleosis or kissing disease) is caused by the Ebstein-Barr virus. It usually runs its course without complications and heals on its own. The worldwide infection rate is more than 90%.
Definition of
Pfeiffer's glandular fever is a viral infection. It is caused by the Epstein-Barr virus (EBV). The infection is symptomatically similar to tonsillitis, but differs significantly from it in the blood count and blood smear. In terms of the clinical picture, it is an infectious mononucleosis.
Epidemiology
EBV infections are common. The pathogen reservoir for EBV is exclusively humans. Worldwide, the infection rate in adults is between 80 and 95%. In Western Europe, more than 95% of adults up to the age of 30 are infected with EBV or have had an infection. In at least half of cases, the disease is asymptomatic or is mistaken for tonsillitis or a flu-like infection. The peak age is between the ages of 15 and 30. In developing countries, maximum infection is often reached in children between the ages of two and five.
Causes
Pfeiffer's glandular fever is triggered by the Epstein-Barr virus (EBV). The pathogen is one of the gamma herpes viruses and is a DNA virus. It is also known as human herpes virus-4 (HHV-4). A distinction is made between two types, EBV type 1 and EBV type 2, as well as numerous EBV strains that occur regionally. Both can cause Pfeiffer's glandular fever.
Pathogenesis
eBV is usually transmitted orally through saliva. This is where the colloquial name "kissing disease" comes from. However, it can also be passed on by droplet infection when coughing or sneezing. During glandular fever, but also after infectious mononucleosis, almost all patients excrete the virus for weeks to months. An estimated 20-30% of infected people remain active shedders for the rest of their lives, even if they are neither symptomatic nor ill.
After a person has been infected with EBV via contaminated saliva, it takes between one and seven weeks for symptoms to appear. Young people usually fall ill within ten to 14 days, while adults generally incubate for four to eight weeks before the first symptoms appear. The viruses first infect the tonsils (lymph nodes in the throat) and infect the B lymphocytes stationed there. These migrate out of the lymph nodes and spread the virus throughout the body, especially in the liver and spleen. The infected B lymphocytes multiply and form so-called memory B cells in the bloodstream. If the infection is acute, infectious mononucleosis additionally stimulates the B cells. Heterophilic antibodies are produced and "immunological chaos" ensues.
The immune system recognizes the rapidly dividing, infected B cells, attacks them with large, atypical, mononuclear CD8+ cells and natural killer cells (NK cells) in the blood and lyses them. In order to escape the immune system, the EBV produces virus-encoded IL-10, which inhibits the activity of the NK cells and the cytotoxic T lymphocytes. This allows the infected B lymphocytes to reinfect the epithelium in the oral cavity and the parotid gland during the course of the disease. The classic symptoms of mononucleosis develop.
Symptoms
The younger the affected patients are, the more often the initial infection is asymptomatic. Children under the age of five usually show no symptoms at all or unspecific signs of an upper respiratory tract infection with a high fever and bright red throat. older patients more frequently develop full acute infectious mononucleosis. In adults, the symptom triad of febrile angina tonsillaris (sore throat) and pharyngitis ("raw throat") plus swelling of the lymph nodes and the typical blood count with absolute and relative lymphocytosis with atypical lymphocytes, the so-called virocytes, is characteristic.
In addition, the spleen may be enlarged in around 50% of cases (splenomegaly). Caution is advised here, as the enlargement of the spleen can be so fulminant that it ruptures and the spleen ruptures. Swelling of over 500 g is possible.
Other symptoms may include
- hepatitis with jaundice (icterus) => in about 5% of cases
- Rhinitis
- Cough
- Tearing of the eyes
- Skin rash
- Meningitis (inflammation of the meninges) with photophobia
- Sore throat, headache, aching limbs and muscles
- general feeling of exhaustion and fatigue
- Meningoencephalitis (inflammation of the brain and meninges)
- Myalgia
- Polyneuritis
- Guillain-Barré syndrome
- Exanthema thrombocytopenia
- Myocarditis
- Pericarditis
- interstitial pneumonia (lung inflammation)
- Glomerulonephritis
- Hairy leukoplakia
In addition to classic Pfeiffer's glandular fever, EBV infections can also be chronic in individual cases. Chronic acute EBV infection is characterized by repeated episodes of fever, splenomegaly, hepatitis, viral pneumonia, swelling of the lymph nodes and arthralgia. Chronic fatigue syndrome can also be triggered by EBV.
Diagnosis
The clinical picture of Pfeiffer's glandular fever is relatively impressive with the triad of symptoms and the diagnosis is often made on the basis of the clinical picture. However, as many infections can be asymptomatic or present with a myriad of other symptoms and closely resemble other clinical pictures, other differential diagnoses should also be considered. These include common streptococcal angina, acute HIV disease, angina plaut vincenti, diphtheria, cytomegalovirus infections, agranulocytosis and acute leukemia. It is important to also consider Pfeiffer's glandular fever in the case of possible streptococcal angina. Streptococcal angina is usually treated with aminopenicillins. If these are mistakenly administered for Pfeiffer's glandular fever, a drug exanthema may occur. Aminopenicillins are therefore contraindicated in EBV infections.
Laboratory
EBV is detected in the laboratory. Lactate dehydrogenase (LDH) and transaminases may be elevated in the blood. If the Wolf quotient (lymphocyte/leukocyte count) is greater than 0.35, this also indicates infectious mononucleosis. Lymphocytosis with 40-90% atypical lymphocytes can be easily recognized in the blood smear. So-called Pfeiffer cells are also present. These virocytes are activated cytotoxic T lymphocytes.
In addition to the blood test, antibodies for an EBV infection are also detected serologically in the laboratory. In an acute EBV infection, the antibodies against viral capsid antigen (anti-VCA) of the IgM and IgG type are elevated, antibodies against the Eppstein-Barr virus nuclear antigen (anti-EBNA-1 (IgG)) are negative. The Paul-Bunnel reaction in the rapid test can also provide rapid information. The test is positive in 80% of adults, but only in half of children. Only the serological laboratory test provides definitive proof. A previous EBV infection can be distinguished from a recent infection by positive anti-VCA p18 IgG and anti-EBNA-1 IgG values. In this case, anti-EBV-VCA and anti-EBV-EA are negative.
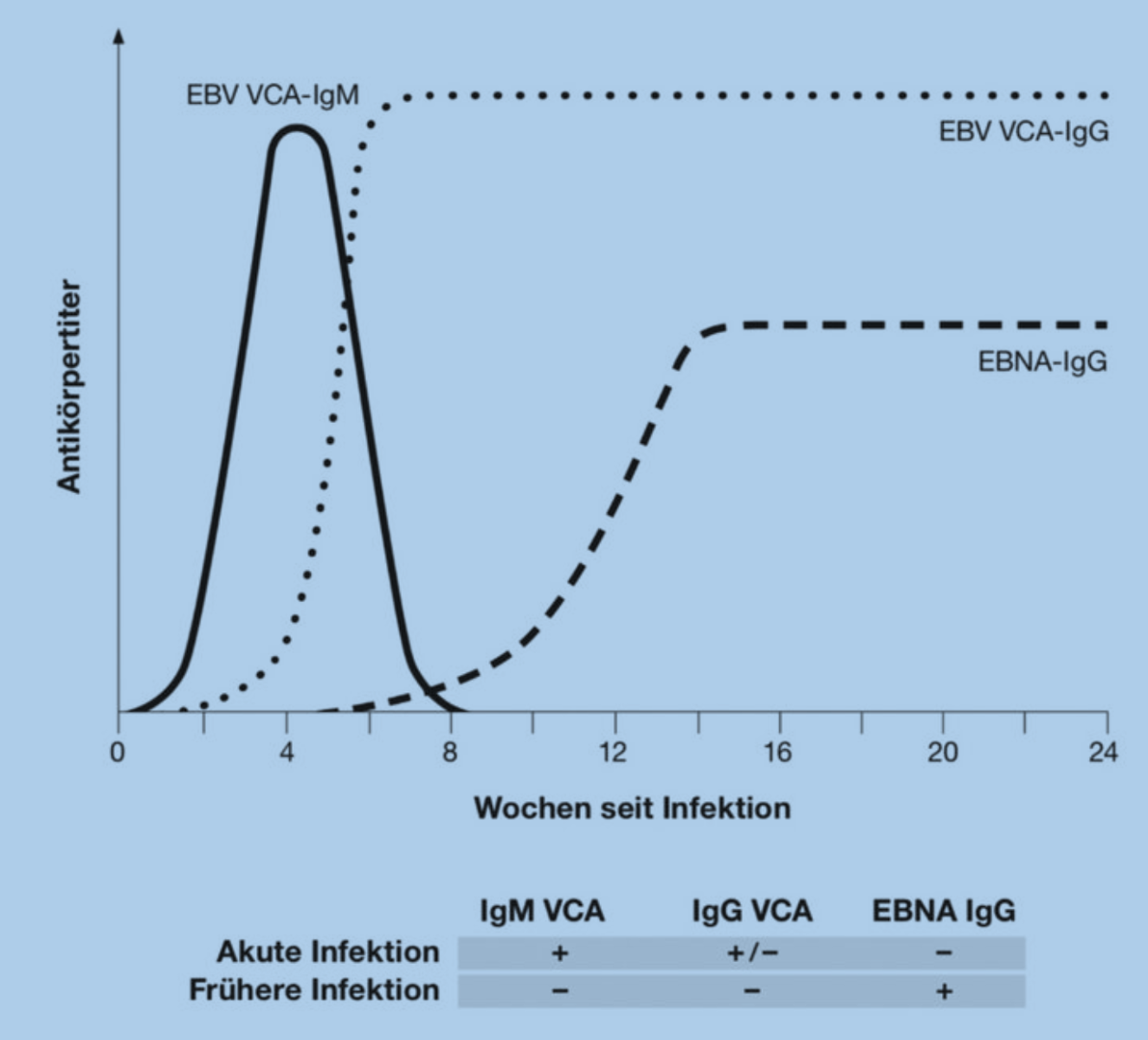
EBV serology in infectious mononucleosis.
Therapy
As with many viral diseases, Pfeiffer's glandular fever is treated exclusively symptomatically. Sufferers should take it easy physically for at least six weeks, drink plenty of fluids and, if necessary, take antipyretics and painkillers such as paracetamol. In severe cases or with complicating additional symptoms, hospitalization may be necessary. The treatment then depends on the additional symptoms.
If hair leukoplakia occurs as part of the EBV infection, treatment with acyclovir can be tried.
Prognosis
Pfeiffer's glandular fever usually heals without complications in immunocompetent patients. However, it is protracted. Immunocompromised patients can have severe courses and be hospitalized.
In individual cases, complications or secondary diseases can occur. These include the very rare rupture of the spleen due to swelling of the spleen (splenomegaly). It requires acute treatment and can be fatal. Kidney failure and peri- or myocarditis can also occur. If other secondary diseases and complications such as Guillain-Barré syndrome, meningoencephalitis or infection-associated haemophagocytic syndrome occur, the prognosis depends on these secondary diseases and complications.
Men with a congenital X-linked lymphoproliferative syndrome have a poor prognosis, as they often develop severe courses of mononucleosis. In the acute stage, the mortality rate is around 70%.
Further complications of EBV infection are associated malignancies or EBV-associated tumors. In Africa, EBV probably triggers all cases of endemic Burkitt's lymphoma, a non-Hodgkin's lymphoma. Worldwide, it occurs only sporadically and is associated with EBV in about 15% of cases. Other associated malignancies are transplant-associated B-cell lymphoma with a poor prognosis, nasopharyngeal carcinoma, Hodgkin's disease and oral hairy leukoplakia, which mainly occurs in HIV patients.
Prophylaxis
EBV is transmitted by droplet infection. To prevent infection, contact with people who are acutely ill should be avoided and, above all, physical contact should be avoided. There is currently no vaccination against EBV.
Hints
Pfeiffer's glandular fever is caused by EBV and is transmitted by droplet infection. In very rare cases, the swelling of the spleen can lead to a ruptured spleen and EBV is similar in symptoms to tonsillitis. If it is not clear whether it is tonsillitis or an EBV infection, a swab should first be taken before antibiotics are prescribed. If ampicillin or amoxicillin are mistakenly given for an EBV infection, a drug exanthema may occur.
Conclusion
- Typical clinical findings of infectious mononucleosis (IM) include sore throat, lymphadenopathy, fever, fatigue, splenomegaly or liver enlargement, jaundice and purulent tonsillar plaques. These symptoms occur mainly in patients aged between 10 and 30 years, and around 15% of patients with infectious mononucleosis (IM) present with an atypical clinical picture, for example with only fatigue. typical laboratory findings in infectious mononucleosis (IM) are elevated transaminases (in 80% of patients) and lymphocytosis (in around 70%). Serologic tests should be performed in the first few weeks to date and assess the association of symptoms with IM. EBNA IgG antibodies appear at the earliest eight to twelve weeks after the onset of symptoms and persist for life.Infectious mononucleosis (IM) occasionally occurs in adults over the age of 40.
25% of patients are still tired six months after the onset of symptoms. Early encouragement and an adapted exercise program can promote recovery.
Due to the risk of spleen rupture, exercise should be avoided for three to six weeks, regardless of the clinically determined spleen size.
Infectious mononucleosis (IM) is not highly contagious. Special hygiene measures are therefore not necessary and often unrealistic, as the virus can be shed for several months.