Singultus, more commonly known as hiccups, is a sudden and uncontrollable contraction of the diaphragm. This causes the glottis to close quickly and produces the typical "hiccup" sound.
Definition
Singultus (Latin: sobbing, gasping), also known as hiccups in common parlance, is usually a short-term symptom with no pathological value. It is a reflexive inhalation movement with simultaneous closure of the vocal folds. If the singultus persists over a longer period of time, in addition to the significant reduction in quality of life, it can be caused by serious diseases of various organ systems, which require a differentiated, but also interdisciplinary diagnostic clarification.a distinction is made depending on the duration of the singultus
- Singultus attack lasting up to 48 hours
- chronic singultus >48 h up to one month
- Therapy-refractory singultus >1 month
Pathophysiology
The physiological and pathophysiological significance of singultus is still not understood down to the last detail. Singultus-like movements of the fetus can be perceived by the mother as early as the 8th week of pregnancy. Singultus in infancy is very common after feeding, whereas it decreases significantly with increasing age, but never disappears completely. singultus is generally assumed to be a disorder in the swallowing reflex arc, in which the phrenic nerve, vagus nerve, brain stem and sympathetic nervous system are involved. the reflex arc can be divided into 3 parts:
- Afferent limb: composed of the fibers of the vagus and phrenic nerves and the thoracic parts of the sympathetic nervous system from Th 6-Th 12.
- Central connection: Assuming a swallowing center independent of the respiratory center, the brain stem and hypothalamus are interconnected with the involvement of the various cranial nerve nuclei.
- Efferent limb: Innervation of the diaphragm by the phrenic nerve, the anterior scalene muscles (C5-C/7), intercostal muscles and innervation of the glottis by the recurrent branch of the vagus nerve.
The diaphragmatic contraction that occurs during hiccups generally occurs unilaterally, usually on the left, although bilateral occurrence is possible. After the diaphragmatic contraction begins, the glottis closes, promptly ending inspiration and producing the characteristic "hiccuping" sound. Today, it is assumed that singultus is a gastrointestinal reflex that is associated with a reduction in oesophageal peristalsis and the tone of the lower oesophageal sphincter with increased acid reflux. Both changes normalize after the attack of singultus.
Epidemiology
Exact data on the prevalence and incidence are not available, as singultus is a symptom with different underlying diseases. It is assumed that males and females are equally affected by transient singultus, while males predominate in chronic singultus. The peak age of chronic singultus in men is between the 6th and 8th decade, while that of women is in the 4th decade.
Clinic
A basic distinction is made between acute and chronic singultus, with the latter lasting for more than 48 h or recurring, and episodes of singultus occurring most frequently in the evening. Although singultus can occur in any phase of the respiratory cycle, it occurs most frequently during inspiration. The singultus frequency can be very stable in patients, but varies greatly between individuals between 2-60/min. Singultus can also occur during sleep, although sleep generally has an inhibitory effect.
Diagnostics
The diagnosis is aimed at the possible multiple causes of singultus, whereby several specialist disciplines often have to be involved in the sense of interdisciplinarity. According to etiological aspects, a classification is possible as follows:
- peripheral or
- central nervous
- infectious
- medicinal
- metabolic
- psychogenic
- idiopathic
Acute singultus in healthy people is usually self-limiting and requires no further diagnosis. Acute distension of the stomach, certain foods or spices or even excessive alcohol consumption can trigger acute singultus, and the diagnosis of singultus begins with a detailed medical history, which should include the following aspects
- the timing of the singultus episodes
- Persistence of the singultus during sleep
- Accompanying symptoms (gastrointestinal, respiratory, etc.)
- Influence of the singultus through appropriate maneuvers
- previous operations
- Alcohol and drug consumption
This is followed by a physical examination, which includes in particular the thorax, the gastrointestinal tract, the nervous system, the urinary tract and the ear, nose and throat area, and further instrumental diagnostics are based on the suspected causes of chronic singultus, which are summarized in Table1.
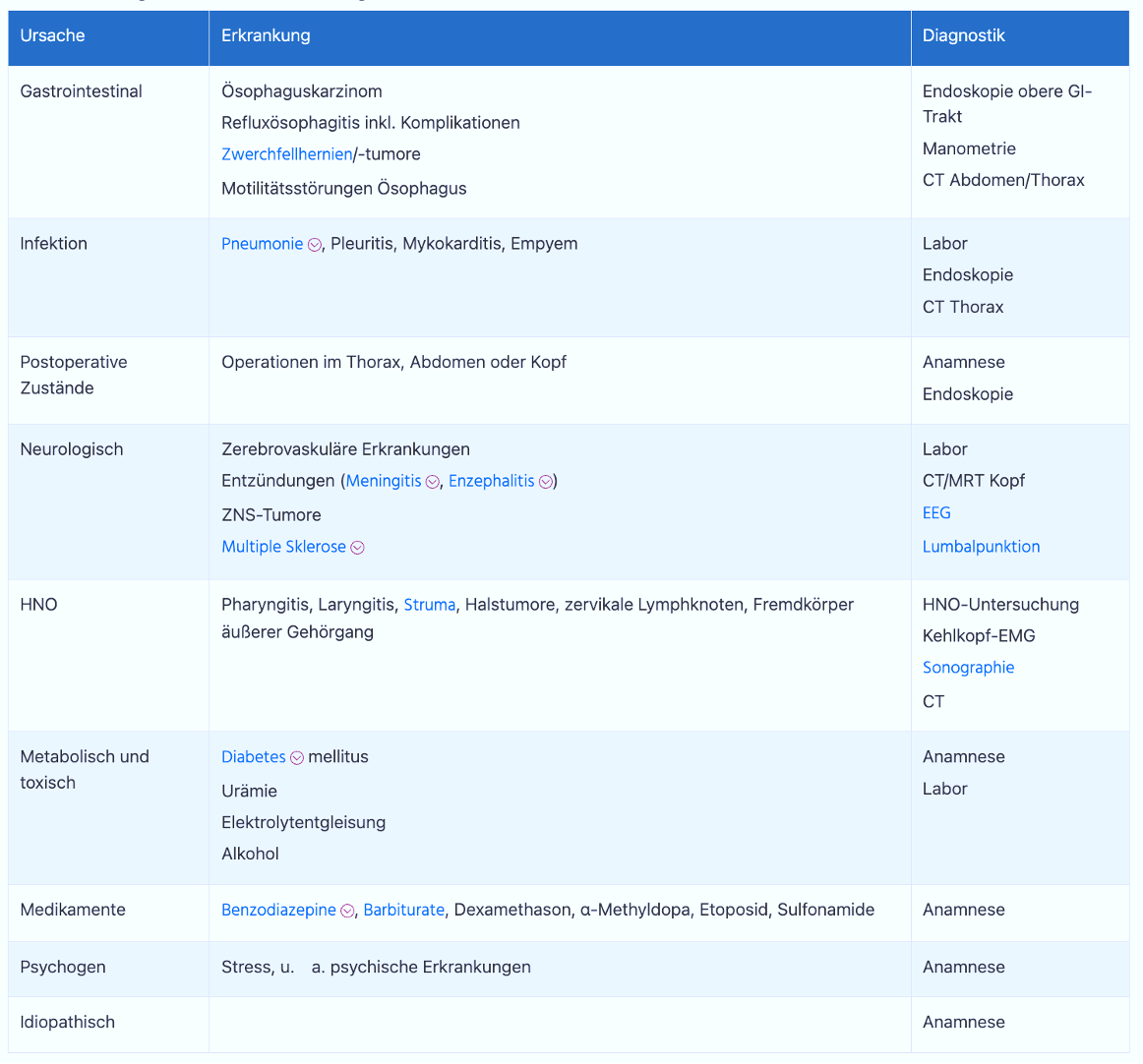
Cause and diagnosis of chronic singultus
Chronic singultus is often caused by a gastrointestinal disease without this always leading to further gastrointestinal symptoms. This applies in particular to esophageal diseases such as gastroesophageal reflux disease, although the causal relationship can only be proven by treating the underlying disease with simultaneous improvement of the singultus. If singultus occurs after a surgical procedure, complications such as peritonitis or subphrenic abscesses must be ruled out. If the singultus persists during sleep, an organic cause is likely and requires consistent diagnostics.
Therapeutic options
The treatment of chronic singultus always focuses on treating the underlying disease. If no cause is found in the diagnosis, non-pharmacological and pharmacological treatments are possible; non-pharmacological therapy includes respiratory maneuvers, nasal and pharyngeal stimulation and vagal stimulation. Behavioral therapies and hypnosis are also used successfully. Pharmacotherapeutic options are available if the non-drug therapies do not lead to a lasting response. Baclofen is the treatment of choice for chronic singultus, usually also in combination with a proton pump blocker or a prokinetic in the presence of an oesophageal or gastric cause of the singultus. The drug treatment options with the corresponding dosages are summarized here.
Drug therapy options for singultus
Drug
- Baclofen
- Metoclopramide
- Amitriptyline
- Carbamazepine
- Haloperidol
- Nifedipine
- Chlorpromazine
What can you do yourself?
You can try to stop a hiccup with the following measures:
- Hold your breath
- Valsalva maneuver: take a deep breath, hold your nose and force the air into your blocked nose
- Breathe in and out of a paper bag for a while
- Drink a glass of ice water quickly
Acute hiccups will go away on their own after a few minutes, even without any action.